Overview
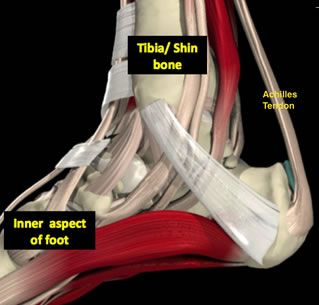 The Achilles tendon is the thickest and strongest tendon in the human body. It plays a very important role in most sport activities and is particularly vulnerable to overloading from repetitive running and jumping. The Achilles tendon forms a joint distal tendon for the gastrocnemius and the soleus muscles. These muscles combine to form the triceps surae muscle. Athletes who sustain Achilles tendon ruptures most frequently are those who participate in ball sports that demand rapid changes of direction and quick, reactive jumps (e.g., tennis, squash, badminton, and soccer), in addition to runners and jumpers in track and field. Sometimes a patient with a ruptured tendon has a history of long-term pain localized to the tendon, but more often the rupture occurs without warning. Such ruptures are often caused by degenerative changes in the tendon (tendinosis), usually in the segment of the tendon that has the worst blood supply. This segment extends from 2 to 6 cm proximal to the insertion of the tendon onto the calcaneus.
The Achilles tendon is the thickest and strongest tendon in the human body. It plays a very important role in most sport activities and is particularly vulnerable to overloading from repetitive running and jumping. The Achilles tendon forms a joint distal tendon for the gastrocnemius and the soleus muscles. These muscles combine to form the triceps surae muscle. Athletes who sustain Achilles tendon ruptures most frequently are those who participate in ball sports that demand rapid changes of direction and quick, reactive jumps (e.g., tennis, squash, badminton, and soccer), in addition to runners and jumpers in track and field. Sometimes a patient with a ruptured tendon has a history of long-term pain localized to the tendon, but more often the rupture occurs without warning. Such ruptures are often caused by degenerative changes in the tendon (tendinosis), usually in the segment of the tendon that has the worst blood supply. This segment extends from 2 to 6 cm proximal to the insertion of the tendon onto the calcaneus.
Causes
Repeated stress from a variety of causes is often the cause of Achilles tendon injury. The stress may occur from any of the following. Excessive activity or overuse. Flat feet. Poorly fitting or inadequate shoes. Inadequate warm-up or proper conditioning. Jogging or running on hard surfaces. Older recreational athlete. Previous Achilles tendon injury (tendonitis/rupture). Repeated steroid injections. Sudden changes in intensity of exercise. Use of fluoroquinolone antibiotics (especially in children). Trauma to the ankle. Tense calf muscles prior to exercise. Weak calf muscles.
Symptoms
Patients with an Achilles tendon rupture will often complain of a sudden snap in the back of the leg. The pain is often intense. With a complete rupture, the individual will only be ambulate with a limp. Most people will not be able to climb stairs, run, or stand on their toes. Swelling around the calf may occur. Patients may often have had a sudden increase in exercise or intensity of activity. Some patients may have had recent corticosteroid injections or use of fluoroquinolone antibiotics. Some athletes may have had a prior injury to the tendon.
Diagnosis
Diagnosis is made mostly by clinical examination with a defect usually noted on visual examination and by touching the area. A simple test can be done by squeezing the back of the calf with the foot resting in the air. Normally when squeezing the muscle belly the tendon will shorten causing the foot to move in a downward position. With a rupture this squeezing effect may show no movement of the foot if it is not attached properly. A negative test does not mean there isn't some degree of rupture as some of the tendon fibers may still be attached. Sometimes x-rays, an mri, or an ultrasound can be helpful in determining the extent of the rupture.
Non Surgical Treatment
Initial treatment for sprains and strains should occur as soon as possible. Remember RICE! Rest the injured part. Pain is the body's signal to not move an injury. Ice the injury. This will limit the swelling and help with the spasm. Compress the injured area. This again, limits the swelling. Be careful not to apply a wrap so tightly that it might act as a tourniquet and cut off the blood supply. Elevate the injured part. This lets gravity help reduce the swelling by allowing fluid and blood to drain downhill to the heart. Over-the-counter pain medication is an option. Acetaminophen (Tylenol) is helpful for pain, but ibuprofen (Motrin, Advil, Nuprin) might be better, because these medications relieve both pain and inflammation. Remember to follow the guidelines on the bottle for appropriate amounts of medicine, especially for children and teens.
Surgical Treatment
Surgery will involve stitching the two ends of the tendon together, before placing the leg in a cast or brace. The advantage of having an operation is the reduced chance of the rupture reoccurring, however it will involve the risks associated with any surgical procedure, such as infection.
The Achilles tendon is the thickest and strongest tendon in the human body. It plays a very important role in most sport activities and is particularly vulnerable to overloading from repetitive running and jumping. The Achilles tendon forms a joint distal tendon for the gastrocnemius and the soleus muscles. These muscles combine to form the triceps surae muscle. Athletes who sustain Achilles tendon ruptures most frequently are those who participate in ball sports that demand rapid changes of direction and quick, reactive jumps (e.g., tennis, squash, badminton, and soccer), in addition to runners and jumpers in track and field. Sometimes a patient with a ruptured tendon has a history of long-term pain localized to the tendon, but more often the rupture occurs without warning. Such ruptures are often caused by degenerative changes in the tendon (tendinosis), usually in the segment of the tendon that has the worst blood supply. This segment extends from 2 to 6 cm proximal to the insertion of the tendon onto the calcaneus.Causes
Repeated stress from a variety of causes is often the cause of Achilles tendon injury. The stress may occur from any of the following. Excessive activity or overuse. Flat feet. Poorly fitting or inadequate shoes. Inadequate warm-up or proper conditioning. Jogging or running on hard surfaces. Older recreational athlete. Previous Achilles tendon injury (tendonitis/rupture). Repeated steroid injections. Sudden changes in intensity of exercise. Use of fluoroquinolone antibiotics (especially in children). Trauma to the ankle. Tense calf muscles prior to exercise. Weak calf muscles.
Symptoms
Patients with an Achilles tendon rupture will often complain of a sudden snap in the back of the leg. The pain is often intense. With a complete rupture, the individual will only be ambulate with a limp. Most people will not be able to climb stairs, run, or stand on their toes. Swelling around the calf may occur. Patients may often have had a sudden increase in exercise or intensity of activity. Some patients may have had recent corticosteroid injections or use of fluoroquinolone antibiotics. Some athletes may have had a prior injury to the tendon.
Diagnosis
Diagnosis is made mostly by clinical examination with a defect usually noted on visual examination and by touching the area. A simple test can be done by squeezing the back of the calf with the foot resting in the air. Normally when squeezing the muscle belly the tendon will shorten causing the foot to move in a downward position. With a rupture this squeezing effect may show no movement of the foot if it is not attached properly. A negative test does not mean there isn't some degree of rupture as some of the tendon fibers may still be attached. Sometimes x-rays, an mri, or an ultrasound can be helpful in determining the extent of the rupture.
Non Surgical Treatment
Initial treatment for sprains and strains should occur as soon as possible. Remember RICE! Rest the injured part. Pain is the body's signal to not move an injury. Ice the injury. This will limit the swelling and help with the spasm. Compress the injured area. This again, limits the swelling. Be careful not to apply a wrap so tightly that it might act as a tourniquet and cut off the blood supply. Elevate the injured part. This lets gravity help reduce the swelling by allowing fluid and blood to drain downhill to the heart. Over-the-counter pain medication is an option. Acetaminophen (Tylenol) is helpful for pain, but ibuprofen (Motrin, Advil, Nuprin) might be better, because these medications relieve both pain and inflammation. Remember to follow the guidelines on the bottle for appropriate amounts of medicine, especially for children and teens.
Surgical Treatment
Surgery will involve stitching the two ends of the tendon together, before placing the leg in a cast or brace. The advantage of having an operation is the reduced chance of the rupture reoccurring, however it will involve the risks associated with any surgical procedure, such as infection.
 RSS Feed
RSS Feed
